MP can cause local or referred pain,
tightness, tenderness, popping and clicking, stiffness and
limitation of movement, autonomic phenomena, local twitch
response (LTR) in the affected muscle, and muscle weakness
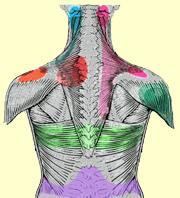
without atrophy. Trigger points (TrPs), which cause referred
pain in characteristic areas for specific muscles, restricted
range of motion (ROM), and a visible or palpable LTR to local
stimulation, are classic signs of MP. Over 70% of trigger points
correspond to acupuncture points used to treat pain.
- In the US: MP is
extremely common, and almost everyone develops a TrP at some time.
In the US, 14.4% of the general population suffers from chronic
musculoskeletal pain. Approximately 21-93% of patients with
regional pain complaints have MP. Studies have demonstrated that
25-54% of asymptomatic individuals have latent TrPs.
Patients usually complain of
regionalized aching and poorly localized pain in the muscles and
joints. They also may complain of sensory disturbance, like numbness
in a similar area of distribution. Onset may be acute after a
specific event or trauma (eg, moving quickly in an awkward position)
or chronic from poor posture or overuse. The type of pain felt is
characteristic of the muscle involved. Patients may note disturbed
sleep and may have been through the "great pillow search" to try to
find a comfortable sleeping position. They may or may not be aware
of muscle weakness in the affected muscles and may have a tendency
to drop things.
A Physiatrist can provide accurate
diagnosis of MP. Unfortunately, most medical school and residency
training programs do not cover this common condition adequately.
Locating TrPs is the most important part of the physical
examination. TrPs tend to occur in characteristic locations in
individual muscles. Travell and Simons' Myofascial Pain and
Dysfunction. The Trigger Point Manual is considered the
criterion standard reference on locating and treating TrPs.
Causes: Several factors
contribute to MP. Abnormal stresses on the muscles from sudden
stress on shortened muscles, leg-length discrepancies, or skeletal
asymmetry are thought to be common causes of MP. Poor posture also
may serve to cause MP. Assumption of a static position for a
prolonged period of time also has been implicated in MP. Anemia and
low levels of calcium, potassium, iron, and vitamins C, B-1, B-6,
and B-12 are believed to play a role. Chronic infections and sleep
deprivation have been cited as causative factors, as have
radiculopathy, visceral diseases, and depression. Hypothyroidism,
hyperuricemia, and hypoglycemia also have been implicated in MP.